



Sponsored Article
The Ultimate Primer on Top Surgery and Nipples
When planning for Top Surgery and solidifying your surgery goals, you might be surprised at the dizzying array of options that you have surrounding... nipples! From Top Surgery techniques, nipple size, shape and placement to post-op sensation, pigmentation and no-nipple options, there are a number of variables to be aware of. This all-about-nipples primer will help you understand your options and their implications, and guide you to decisions that will satisfy your needs.
NAC 101
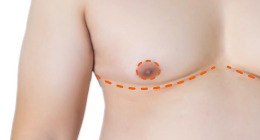
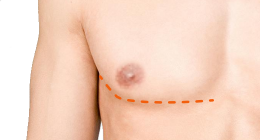
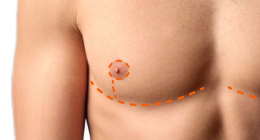
The nipple-areola complex, or NAC, is comprised of both the nipple and the surrounding tissue called the areola. Both the nipple and areola have target sizes, shapes and positioning. The characteristics of an "ideal" male NAC are smaller, more oval than round and positioned more on the outside of the chest compared to the female NAC. [1] The extent to which the NAC can be resized, reshaped and repositioned varies by Top Surgery technique:
- Keyhole - The areola is not resized, but nipple size can be reduced; native NAC shape and positioning are maintained.
- Peri-Areolar - Both the nipple and areola size can be reduced but this is often done in a revision surgery; NAC shape can be optimized to an extent; native positioning of the NAC is maintained.
- Double Incision with Free Nipple Grafts - Offers the most flexibility for NAC size, shape and positioning.
Discussions about reshaping and repositioning the NAC generally refer to Double Incision Top Surgery.
Free Nipple Grafts Explained
Free nipple grafts are full-thickness skin grafts that are used to reconstruct the NAC in Double Incision Top Surgery. The NAC is removed, resized and then grafted back on to the chest after the breast tissue has been surgically removed.
 Despite
the name, free nipple grafts are not actually FREE!
In fact, they may cost you extra. Aetna
and United HealthCare have been denying insurance claims for free
nipple grafts ruling that they are cosmetic and serve no
functional purpose. At the same time, free nipple grafts are
deemed medically necessary and are covered when cis gender women
have mastectomy to prevent or treat breast cancer. Citing that
free nipple grafts are an "inherent and irrefutable part" of Top
Surgery, Dr. Scott
Mosser, one of the most popular and experienced
Top Surgery surgeons in the U.S., co-authored this
letter to spread awareness around the importance of
insurance companies covering free nipple grafts.
Despite
the name, free nipple grafts are not actually FREE!
In fact, they may cost you extra. Aetna
and United HealthCare have been denying insurance claims for free
nipple grafts ruling that they are cosmetic and serve no
functional purpose. At the same time, free nipple grafts are
deemed medically necessary and are covered when cis gender women
have mastectomy to prevent or treat breast cancer. Citing that
free nipple grafts are an "inherent and irrefutable part" of Top
Surgery, Dr. Scott
Mosser, one of the most popular and experienced
Top Surgery surgeons in the U.S., co-authored this
letter to spread awareness around the importance of
insurance companies covering free nipple grafts.
While free nipple grafts offer the most flexibility for NAC sizing, shape and positioning, there are some disadvantages: graft loss, nipple flattening and depigmentation, all of which are discussed later in this article.
Reconstruction of the NAC has been widely discussed with regard to Gynecomastia surgery in cis gender men, but the same cannot be said about NAC reconstruction in the context of Top Surgery. As a result, surgeons performing Top Surgery have different methods for determining the size, shape and positioning of the NAC.
"There is a significant knowledge gap for the ideal nipple-areolar complex shape, size and location." [2]
Nipple and Areola Size
The male areola and nipple are smaller and the nipple has less projection compared to female NAC dimensions.
| Sex | Areola Diameter | Nipple Diameter | Nipple Projection |
| Female | 40 mm * | 13 mm * | 9 mm * |
| Male | 26.6 mm * | 6.9 mm * | 2.6 mm † |
Note: Data are from Dominic Yue et al.*,[3] and Beckenstein, Windle and Stroup†.[4]
 There
is no significant variance in NAC size according to age, ethnicity
or BMI. [5] However, one study found
that Asian people had a higher nipple width:height ratio compared
to non-Asians and Hispanic people had a larger areola width
compared to non-Hispanics.[6] Gender
surgeon Dr.
Gabriel Del Corral co-authored a study that found
that the average NAC size used by Top Surgery surgeons is 2-3cm in
diameter. [7] While the "ideal" male
areola is approximately 25mm in diameter, tension on the skin
closure can cause the areola to stretch out. To account for this,
some surgeons recommend sizing the areola at 22mm, which is about
the size of a nickel. [8]
There
is no significant variance in NAC size according to age, ethnicity
or BMI. [5] However, one study found
that Asian people had a higher nipple width:height ratio compared
to non-Asians and Hispanic people had a larger areola width
compared to non-Hispanics.[6] Gender
surgeon Dr.
Gabriel Del Corral co-authored a study that found
that the average NAC size used by Top Surgery surgeons is 2-3cm in
diameter. [7] While the "ideal" male
areola is approximately 25mm in diameter, tension on the skin
closure can cause the areola to stretch out. To account for this,
some surgeons recommend sizing the areola at 22mm, which is about
the size of a nickel. [8]
With regard to nipple size with free nipple grafts, defatting of the areola when creating the grafts reduces nipple projection enough that further reduction isn't usually necessary. However, if defatting is done too aggressively, nipple projection in the graft can be completely lost. [9] A 2018 study reported that up to 46% of patients had decreased nipple projection due to too much thinning of the graft. [10]
 Dr. Hope Sherie,
a Top Surgery surgeon in Charlotte NC, reduces the size of the
nipple while leaving it attached to the areola. "Some surgeons
remove the nipple completely and sew the areola and nipple into
place as two separate pieces," she says. "They do, however, have
higher reported rates of nipple loss using that technique."
Dr. Hope Sherie,
a Top Surgery surgeon in Charlotte NC, reduces the size of the
nipple while leaving it attached to the areola. "Some surgeons
remove the nipple completely and sew the areola and nipple into
place as two separate pieces," she says. "They do, however, have
higher reported rates of nipple loss using that technique."
With nipple-sparing Top Surgery techniques, such as Keyhole and Peri-areolar, nipple projection may require surgical intervention as the nipples will not shrink to a male size. Some surgeons perform nipple reduction during the initial surgery but it is often delayed and done as a secondary revision procedure due to blood supply.
 "It
depends on how the nipple/areola looks at the end of the surgery,"
says Dr. Michelle
Lee, a Top Surgery surgeon in Beverly Hills and
star of hit TV show, Dr.
90210. "Sometimes with an aggressive
peri-areola surgery, the blood supply to the nipple looks a
little beat up and doing the nipple reduction might kill the
nipple. I then stage the nipple reduction. If the blood supply
looks good at the end of the case, I will then do the reduction at
the same time."
"It
depends on how the nipple/areola looks at the end of the surgery,"
says Dr. Michelle
Lee, a Top Surgery surgeon in Beverly Hills and
star of hit TV show, Dr.
90210. "Sometimes with an aggressive
peri-areola surgery, the blood supply to the nipple looks a
little beat up and doing the nipple reduction might kill the
nipple. I then stage the nipple reduction. If the blood supply
looks good at the end of the case, I will then do the reduction at
the same time."
Areola Shape
Male areolas tend to be more oval than round and slightly slanted, although this has been disputed. Areola shape may be influenced by physical activity, body composition and even room temperature. [11]
 With
Keyhole Top Surgery, native areola shape is maintained. Areola
shape can be modified to an extent in Peri-Areolar Top Surgery,
although this tends to be done as a revision surgery.
With
Keyhole Top Surgery, native areola shape is maintained. Areola
shape can be modified to an extent in Peri-Areolar Top Surgery,
although this tends to be done as a revision surgery.
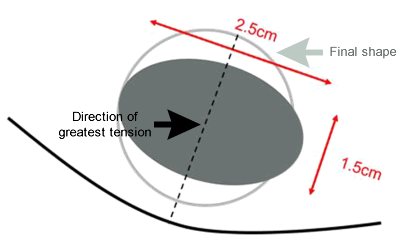
When free nipple grafts are used, most surgeons use a circular shape for the areola. [12] However, the final shape of the areola is largely determined by the dimensions of where the grafts are attached (the recipient site.) Noting this, surgeons in Italy found that modifying the recipient site to an oblique oval shape at the time of grafting addressed the direction of greatest tension and improved aesthetic outcomes. [13]
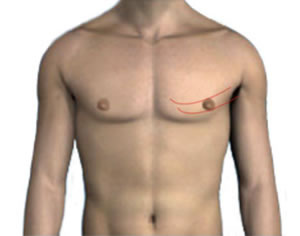
NAC Positioning
On a male chest, the NACs are farther apart compared to a female chest, where NACs are closer to the middle of the chest.
 "It
is very important to place the nipple areola in a masculine
position at the lateral border of the pectoralis muscle," says
Florida-based Top Surgery surgeon Dr.
Russell Sassani. "In a cis gender woman, the
nipple is in the breast meridian, but in a cis gender male, the
nipple areola is laterally placed on the pec. These aesthetic
insights will give the optimal outcome to achieve the best result
for chest masculinization."
"It
is very important to place the nipple areola in a masculine
position at the lateral border of the pectoralis muscle," says
Florida-based Top Surgery surgeon Dr.
Russell Sassani. "In a cis gender woman, the
nipple is in the breast meridian, but in a cis gender male, the
nipple areola is laterally placed on the pec. These aesthetic
insights will give the optimal outcome to achieve the best result
for chest masculinization."
However, there is no consensus among surgeons as to the
best practice for positioning the NAC.
A 2009 study suggested a method for NAC re-positioning that makes use of the "Golden Ratio," also known as the "Divine Proportion."
The Vitruvian Man is a drawing made by Leonardo da Vinci in about 1490. It was created for "De Divina Proportione" (On the Divine Proportion), a book about mathematics that was first published in 1509.
"Currently available guidelines create areolas that are too large, place the nipple-areola complex too high and too far medially, and/or require complex abstract mathematical calculations. Relying on the recently appreciated aesthetic value of the golden number Phi (?) we propose an easy and reliable method to determine the horizontal and vertical coordinates of the male nipples." [14]
 Some surgeons rely on the alignment of various physical landmarks,
such as the borders of the chest muscles. However, this can be
challenging to assess accurately, especially in patients with a
higher BMI. [15]
Some surgeons rely on the alignment of various physical landmarks,
such as the borders of the chest muscles. However, this can be
challenging to assess accurately, especially in patients with a
higher BMI. [15]
Dr. Jonathan Keith, a gender surgeon in New Jersey, says that the NAC can end up being positioned too high and/or too close to the center of the chest when surgeons rely solely on aesthetic intuition. [16] Dr. Keith has developed a three-step technique for optimal NAC positioning in transgender chest masculinization. [17]
1. The vertical coordinate is determined at the level of the 4th rib near the lateral border of the pectoralis muscle.
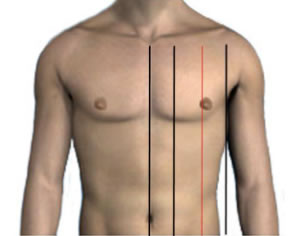
2. The horizontal coordinate is determined by dividing each unilateral chest into vertical thirds from midline to anterior axillary line. The NAC position is confirmed at the junction of the middle and lateral third.
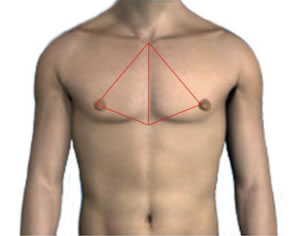
3. Symmetry is ensured bilaterally by creating a triangle; the base lies from sternal notch to inframammary fold in the midline and the apex is adjusted to the NAC. This apex is transposed from side to side to ensure symmetry.
"I'm over the moon with my results. Dr. Sean Herman took into consideration what I wanted my chest to look like as far as scar shape and placement, and nipple/areola size and shape as well. Everything turned out neat and symmetrical, and especially important for me, very natural looking." - RM, Top Surgery patient.
Nipple Sensation
Retaining sensation in the NAC is very important to many people considering Top Surgery but little has been written on the subject. Academic studies on Top Surgery are primarily focused on visual results and complication rates, leaving the topic of sensation to the realm of anecdotal reports on the Internet.
"There are relatively minimal data regarding nipple sensation after surgery... The lack of outcome responses beyond a generic "none, decreased, or unchanged" further potentiates the current knowledge gap." [18]
"Sensation in a nipple graft is not guaranteed," says Dr. Sherie. "I have found that over time most patients regain sensation which feels much like the surrounding chest skin, or slightly decreased, as the graft is innervated by the ingrowth of new nerves. This process may take months to years."
With regard to erogenous sensation, Dr. Sherie says that most patients do not regain the hypersensitivity which some people have in their nipples. "On the other hand, I have had a very small number of patients who had little nipple sensation preoperatively and have actually reported more sensation following a graft, which just demonstrates that ultimately nerves are somewhat unpredictable."
In nipple-sparing Top Surgery techniques, including Keyhole, Peri-Areolar, Inverted-T and Buttonhole, the NAC is left attached to a dermis (deep skin layer) pedicle, which carries blood supply to the NAC and also includes nerves. Provided that there are no nipple healing issues, more sensation is retained or regained with these techniques compared to Double Incision.
 Dr. Paul Steinwald pioneered the Inverted-T method of chest masculinization in which the nipple in most cases can remain attached and therefore retain a degree of sensitivity that is just not possible with free nipple grafts. "Patients often report retention of at least 60-80% of preexisting nipple sensation," says Dr. Steinwald.
Dr. Paul Steinwald pioneered the Inverted-T method of chest masculinization in which the nipple in most cases can remain attached and therefore retain a degree of sensitivity that is just not possible with free nipple grafts. "Patients often report retention of at least 60-80% of preexisting nipple sensation," says Dr. Steinwald.
Post-Operative Healing of the NAC
With nipple-sparing Top Surgery techniques, there is minimal post-operative management of the NAC. Patients are instructed to apply petroleum jelly products, usually Vaseline or Aquafor, or Polysporin/Bacitracin, and place fresh dressings on incisions daily.
With Double Incision Top Surgery, the free nipple grafts are fixed into place with a "tie-over dressing" of Xeroform gauze folded up in a ball. Often referred to as a bolster, this moist dressing creates continuous compression of the graft against the recipient site to immobilize it, prevent shearing/straining, and prevent hematoma or seroma formation under the graft. [19]
The bolsters are removed by the surgeon after 5-7 days and the patient is instructed to cover the nipple grafts with a non-adherent dressing (eg, Telfa) treated with Aquaphor or Vaseline for another 2 weeks. The new NAC eventually darkens with pigmentation over the next 3-9 months.
WATCH NOW: Dr. Drew Schnitt demonstrates the removal of nipple graft bolsters.
 It can take up to a year or more
until the free nipple grafts are fully healed and redness around
the areolas disappears. While the grafts are healing,
they can start looking worse before they look better,
especially around 2-3 weeks after surgery. This is because in
reality, only a portion of the graft survives. San Francisco
gender surgeon Dr.
Dev Gurjala explains:
It can take up to a year or more
until the free nipple grafts are fully healed and redness around
the areolas disappears. While the grafts are healing,
they can start looking worse before they look better,
especially around 2-3 weeks after surgery. This is because in
reality, only a portion of the graft survives. San Francisco
gender surgeon Dr.
Dev Gurjala explains:
"All that's really important is that the deepest layer of cells in contact with the vascular bed survives. Over time, the deeper layers of cells push off or slough the more superficial layers, which are acting as a 'biologic' dressing for the deeper layers to heal and proliferate. This is why NAC grafts can often look so scary and induce anxiety—what is visible is the superficial layers which are devitalized, but doing their job as a protective covering, and are meant to slough off over a few weeks time. The sloughing is often interpreted as loss of the graft or as infection when in reality nipple graft loss is actually quite rare."
 This
sloughing off is medically referred to as desquamation.
Seattle-area Top Surgery surgeons, Dr.
Alvina Won and Dr.
Tony Mangubat, found that patients often have
concerns and questions during the healing process about what to
expect, especially during the desquamation period.
This
sloughing off is medically referred to as desquamation.
Seattle-area Top Surgery surgeons, Dr.
Alvina Won and Dr.
Tony Mangubat, found that patients often have
concerns and questions during the healing process about what to
expect, especially during the desquamation period.
"Providing education and information about the healing process of free nipple grafts will help to reassure the patients as well as their caregivers," says Dr. Won. [20]
To ease concerns during this vulnerable period of recovery, Dr. Mosser created this helpful visual breakdown of what most NACs look like from 7 days after Top Surgery all the way up to 3 months.
The NAC and Pigmentation
Although the NAC can range in color, it generally tends to be paler in females and darker in males. Depigmentation of the NAC occurs in up to 42% of patients undergoing a free nipple graft, and even when successful, nipple grafts do not address the color variations in female and male NACs. [21]
NAC pigmentation is produced by certain types of cells called melanocytes. When a free nipple graft is healing, it takes time for the melanocytes to increase in number and start producing pigment again.
"I always tell my patients that it will take about a year or two for the pigment to evenly return—to expect this, not be surprised by it, and give the body time to do its thing," says Dr. Gurjala.
If there are complications while the grafts are healing, the end result will have more scarring, which appears as whitish or pinkish in color, and there will be less melanocytes to produce enough pigment for even coloration. If pigmentation does not fully return, tattooing of the depigmented areas can produce excellent results.
Tattooing can also be helpful in cases where the NAC has stretched out of shape. There is a tendency for the grafted NACs to stretch in a vertical direction over time due to skin tension, especially if the recipient site was not created in a more oval shape. [22]
No Nipples
A growing trend in Top Surgery is opting for no NAC. There are several reasons why someone might want to have a NAC-free chest:
- Some people simply like the aesthetic of a more non-binary result;
- Some people find nipple sensation to be dysphoric, too sensory;
- Better control over NAC size, shape, positioning and pigmentation with tattooing;
- Insurance not covering nipple grafts;
- Worry about graft loss;
- Have diabetes, vascular or autoimmune conditions.
With Double Incision Top Surgery, you can ask your surgeon to not perform the NAC reconstruction, resulting in a smooth, nipple-free chest.
Keep in mind: Not all surgeons will do this.
 Dr. Daniel Medalie,
an experienced Top Surgery surgeon in Ohio, does not offer a
NAC-free Top Surgery. "Nipples are part of the normal human
anatomy and I am only comfortable performing surgery to create
natural results," he says. "Additionally the nipple/areolar
complex is unique and can't be reconstructed once thrown away." [23]
Dr. Daniel Medalie,
an experienced Top Surgery surgeon in Ohio, does not offer a
NAC-free Top Surgery. "Nipples are part of the normal human
anatomy and I am only comfortable performing surgery to create
natural results," he says. "Additionally the nipple/areolar
complex is unique and can't be reconstructed once thrown away." [23]
According to one study, graft loss occurred in up to 18% of patients undergoing free nipple grafting. [24] However, Dr. Mosser says that it is extremely rare to lose a considerable portion of a skin graft for any reason, and he has not had a patient completely lose any of the hundreds of nipple grafts performed. [25]
Dr. Sherie agrees. "To date in our practice, the risk of partial nipple loss with a nipple graft procedure is 0.3%, or a little less than one in 3,000."
Risk factors for nipple graft loss include smoking (nicotine, cannabis), diabetes and vascular or autoimmune conditions.
For those who choose to forgo NAC reconstruction, prosthetics are an option for those days when you do feel like having NACs. Prosthetic NACs can increase personal safety in public places where you would go shirtless, such as a beach or a public swimming pool. GenderCat's prosthetic NACs are waterproof.
There are many things to consider when planning for Top Surgery and this includes making decisions about how you would like your nipples and areolas to turn out—if you want nipples and areolas at all! Armed with the information in this all-about-nipples primer, you can feel confident about going into a Top Surgery consultation and having a detailed, high-level conversation with your prospective surgeon about how the various NAC options fit into your surgery goals.
References
1. Frey JD, Yu JZ, Poudrier G, Motosko CC, Saia WV, Wilson SC, Hazen A. Modified Nipple Flap with Free Areolar Graft for Component Nipple-Areola Complex Construction: Outcomes with a Novel Technique for Chest Wall Reconstruction in Transgender Men. Plast Reconstr Surg. 2018 Aug;142(2):331-336. doi: 10.1097/PRS.0000000000004551. PMID: 29794642.
2. Cohen WA, Shah NR, Iwanicki M, Therattil PJ, Keith JD. Female-to-Male Transgender Chest Contouring: A Systematic Review of Outcomes and Knowledge Gaps. Ann Plast Surg. 2019 Nov;83(5):589-593. doi: 10.1097/SAP.0000000000001896. PMID: 31082837.
3. Dominic Yue, MRCS, Lilli R L Cooper, MRCS, Ryan Kerstein, MRCS, Susan C Charman, MSc, Norbert V Kang, MD, FRCS, Defining Normal Parameters for the Male Nipple-Areola Complex: A Prospective Observational Study and Recommendations for Placement on the Chest Wall. Aesthetic Surgery Journal, Volume 38, Issue 7, July 2018, Pages 742–748.
4. Beckenstein MS, Windle BH, Stroup RT Jr. Anatomical parameters for nipple position and areolar diameter in males. Ann Plast Surg. 1996 Jan;36(1):33-6. doi: 10.1097/00000637-199601000-00007. PMID: 8722981.
5. Dominic Yue et al.
6. Agarwal CA, Wall VT, Mehta ST, Donato DP, Walzer NK. Creation of an Aesthetic Male Nipple Areolar Complex in Female-to-Male Transgender Chest Reconstruction. Aesthetic Plast Surg. 2017 Dec;41(6):1305-1310. doi: 10.1007/s00266-017-0935-7. Epub 2017 Jul 11. PMID: 28698936.
7. Bustos, S., Kuruoglu, D., Yan, M., Bustos, V., Forte, A., Ciudad, P., Kim, E., Del Corral, G., & Manrique, O. (2020). Nipple-areola complex reconstruction in transgender patients undergoing mastectomy with free nipple grafts: a systematic review of techniques and outcomes. Annals Of Translational Medicine, 0. doi:10.21037/atm-20-4522.
8. Frederick MJ, Berhanu AE, Bartlett R. Chest Surgery in Female to Male Transgender Individuals. Ann Plast Surg. 2017 Mar;78(3):249-253. doi: 10.1097/SAP.0000000000000882. PMID: 27845966.
9. Frederick MJ, Berhanu AE, Bartlett R.
10. Frey JD et al.
11. Agarwal CA et al.
12. Bustos et al.
13. Tanini S, Lo Russo G. Shape, Position and Dimension of the Nipple Areola Complex in the Ideal Male Chest: A Quick and Simple Operating Room Technique. Aesthetic Plast Surg. 2018 Aug;42(4):951-957. doi: 10.1007/s00266-018-1131-0. Epub 2018 Apr 11. PMID: 29644416.
14. Atiyeh, Bishara S. MD, FACS*; Dibo, Saad A. MD†; El Chafic, Abdul Hamid MD‡ Vertical and Horizontal Coordinates of the Nipple-Areola Complex Position in Males, Annals of Plastic Surgery, November 2009 - Volume 63 - Issue 5 - p 499-502 doi: 10.1097/SAP.0b013e3181953854
15. Dominic Yue et al.
16. Cohen, Wess A. MD; Shah, Nikhil R. BA; Iwanicki, Margaret MD; Therattil, Paul J. MD; Keith, Jonathan D. MD, FACS Female-to-Male Transgender Chest Contouring, Annals of Plastic Surgery, November 2019 - Volume 83 - Issue 5 - p 589-593 doi: 10.1097/SAP.0000000000001896
17. Haripriya S Ayyala, MD, Thayer J Mukherjee, MD, Thuy-My Le, MSE, Wess A Cohen, MD, Margaret Luthringer, MD, Jonathan D Keith, MD, FACS. A Three-Step Technique for Optimal Nipple Position in Transgender Chest Masculinization. Aesthetic Surgery Journal, Volume 40, Issue 11, November 2020, Pages NP619–NP625.
18. Cohen et al.
19. Won A and Mangubat EA. Free Nipple Grafts: What to expect during the healing process. The American Journal of Cosmetic Surgery, April 2020, doi:10.1177/0748806820915045.
20. Won A and Mangubat EA.
21. Frey JD et al.
23. Medalie, D. Female to Male Surgery (FtM top surgery). Retrieved from https://www.clevelandplasticsurgery.com/transgender/female-to-male-surgery/. Date accessed: March 2, 2021.
24. Frey JD et al.
25. Mosser, Scott. FTM & FTN Nipple Grafts Retrieved from https://www.genderconfirmation.com/all-about-ftm-nipple-grafts/. Date accessed March 2, 2021.
Last updated: 09/19/23